The Proprioceptive Deep Tendon Reflex (P-DTR) Method was founded and developed by Dr. Jose Palomar and has been successfully used in clinical practice for many years. P-DTR is the first manual neurological therapy based on neurology, neurophysiology, biomechanics, and applied kinesiology principles. It is a neurological reflex system that effectively treats a wide range of functional problems and resolves musculoskeletal, gastrointestinal, hormonal, chemical, and emotional dysfunctions. Dysfunction is considered a physiological and reflex disorder of internal organs, which in most cases has a compensatory nature.
The main goal of P-DTR treatment is to restore optimal reflex activity of the nervous system in response to a stimulus. This includes both motor and glandular responses, which leads to the absence of pain or discomfort symptoms perceived by the patient, optimal range of motion, and appropriate adaptation to external environmental conditions. In other words, neurological health is restored.
P-DTR is a very gentle, non-invasive, and painless method based on the real-time manual effect on specific sensory receptors of the human body. Dr. Palomar created a unique system of neurological challenges and discovered predictable “rules” demonstrating how the central nervous system (CNS) responds to stimuli. He thoroughly demonstrated the difference in CNS response under normal conditions (without dysfunction) and during stimulation of a dysfunctional afferent input.
The types of manual afferent inputs (stimuli) used can be delivered in various ways, including light stroking (to stimulate touch receptors), local stretching (Golgi receptors), deep pressure (Pacini receptors), and others. Today, P-DTR works with most exteroceptors, interoceptors, and proprioceptors that form the afferent input to the CNS.
The physiological explanation behind this method is straightforward: each receptor type (e.g., Golgi, Pacini, vibration, nociceptors) is stimulated, and when the receptor’s threshold is exceeded by the amount of stimulus, these stimuli are converted into electrical impulses. These impulses form the afferent information that reaches the CNS, each input traveling along its respective pathways. The CNS receives, interprets, and produces a motor or glandular response based on the synthesis of all received information. For example, the sensation of pain is synthesized directly in the brain and is a complex product of information from nociceptive, proprioceptive, and exteroceptive systems. In summary, pain is the brain’s interpretation based on a complex integration of information from different sources.
Core principles of the P-DTR concept:
- The CNS controls all functional processes of the body at the physical, biochemical, endocrine, emotional, and mental levels.
- All functional or dysfunctional changes are defined by the CNS.
- The CNS continuously receives and interprets external and internal information.
- Every motor, glandular, or conscious thought response depends on the quality of the information received and its interpretation.
- Aberrant, distorted, or excessive threshold signals from receptors will cause neuromuscular, endocrine, or behavioral dysfunctions.
- The primary cause of dysfunction is aberrant afferent information entering the CNS.
- Neurological dysfunctions can persist indefinitely and affect an individual’s optimal performance (often long after physiological healing from trauma is complete).
- The CNS constantly modulates incoming signals to control afferent flow, enabling the individual to make sense of their environment and respond appropriately.

La méthode P-DTR fournit les outils et les évaluations nécessaires pour localiser et diagnostiquer les récepteurs dysfonctionnels, stimuler toutes les composantes d’une dysfonction, identifier la zone prioritaire la plus importante pour le système nerveux, contrôler le flux d’informations afférentes, et le réinitialiser en cas de dysfonction. Ce processus modifie ainsi l’intégration des stimuli nocifs et la formation même de la sensation de douleur.
Le principe théorique fondamental repose sur l’appariement des signaux afférents dysfonctionnels. Une information afférente excessive provenant des champs de récepteurs appariés, ainsi qu’un changement quantitatif du flux d’informations d’un champ, induisent inévitablement une modification du flux d’informations dans un autre champ. En d’autres termes, tout stimulus provenant d’un récepteur dysfonctionnel est automatiquement compensé par le système nerveux central (SNC).
Un SNC neurologiquement sain et bien organisé reçoit et analyse en continu les informations entrantes pour produire une réponse motrice et/ou glandulaire adaptée. Lorsque les seuils d’activation des récepteurs se situent dans ce que l’on appelle la “zone verte” (zone optimale de fonctionnement), cela signifie que les informations sont maîtrisées, gérées efficacement par le SNC, qui dispose de ressources suffisantes pour l’autocompensation, l’autorégulation et les performances optimales au quotidien. Ces récepteurs sont dits “fonctionnels” et déclenchent leur réponse à un seuil d’action optimal.
À l’inverse, un récepteur “dysfonctionnel” présente un seuil d’action altéré, trop élevé ou trop bas, ce qui le rend énergétiquement inefficace et constitue une source de stress systémique pour le SNC, qui doit compenser cette altération de la fonction normale.
En présence de signaux élevés provenant de tels récepteurs, le SNC choisira toujours de compenser ces signaux, quel qu’en soit le coût pour le corps, ce qui peut entraîner divers dysfonctionnements : maladies, instabilité, amplitude de mouvement limitée, fatigue, troubles émotionnels, etc.
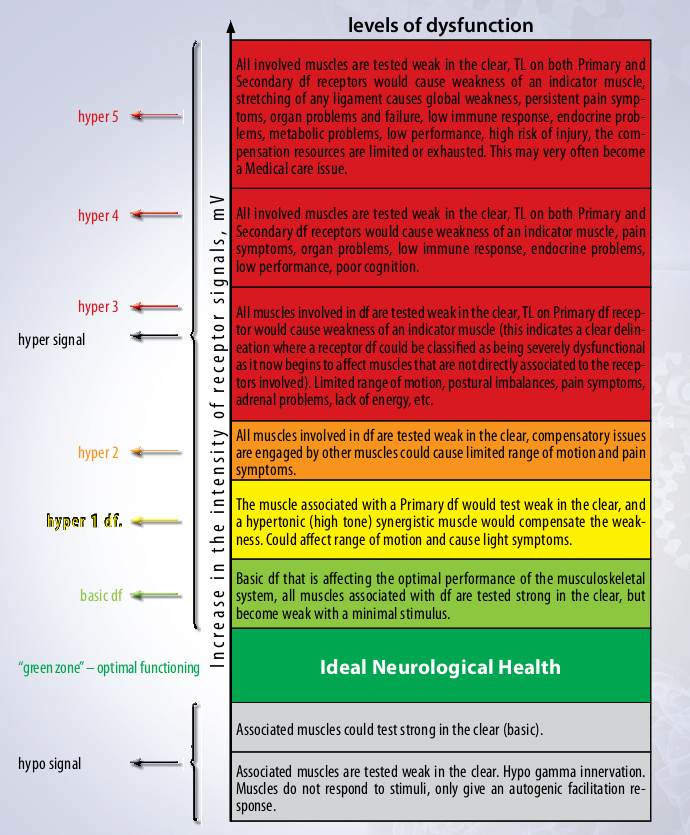
Dr. Palomar thoroughly studied receptors exhibiting aberrantly high signals and discovered that among these dysfunctional receptor fields, one is always prioritized as the primary dysfunctional zone. This field presents a high signal and is consistently compensated by another receptor, designated as the main secondary compensatory zone, which also exhibits an excessive signal. When the compensation provided by this secondary zone is insufficient, the brain creates additional virtual secondary compensations, and if these remain inadequate, it generates new dysfunctions intended to further increase the compensation for the primary priority receptor problem.
Dr. Palomar thus revealed that dysfunctional receptors with high signals can generate fractal compensations, forming a true “compensatory tree” that affects the entire body and may lead to major physiological, endocrine, and immune disorders.
Furthermore, he demonstrated that any dysfunctional signal disrupts the muscle myotatic reflex via the muscle spindle cells, thereby altering the muscular response observable through Manual Muscle Testing (MMT). An aberrant signal originating from any receptor field can cause either a functional weakness or hypertonicity of a single muscle, as well as potentially hypo- or hypertrophic responses on a global scale. Each primary, secondary, or tertiary dysfunctional receptor is associated with specific muscles showing particular inhibition patterns, depending on the central nervous system (CNS) level where the signal is blocked.
Once the primary and secondary dysfunctional receptor fields are located and confirmed, the aberrant afferent flow can be “reset” by simultaneously stimulating these two fields combined with activation of the Deep Tendon Reflex (DTR). This dual stimulation sends two compensatory signals to the CNS, allowing the brain to reset the aberrant information.
Dr. Palomar also discovered that the DTR is not merely a localized reflex as classically described but influences the entire central nervous system and modulates the brain’s neurological response. One possible explanation is that the deep tendon reflex itself acts as a corrective and/or damage control mechanism for the CNS, enabling the brain to promptly assess afferent information and respond appropriately.
During simultaneous stimulation of the primary and secondary fields, the brain receives prioritized information from these specific zones and becomes sensitized to them. The DTR stimulation helps the brain reconstruct and reset the aberrant information, bringing the high signal down into the “green zone,” which corresponds to optimal functioning. The brain then no longer needs to compensate for this signal. In most cases, treatment results are immediate and visible: pain symptoms disappear or greatly diminish, range of motion improves, muscles test as normotonic, and inhibition patterns vanish.
P-DTR also works at different levels of the CNS’s neurological organization. Dr. Palomar applied the same concept of aberrant receptor signals to higher regulatory centers of the CNS and obtained successful results working with cranial nerve nuclei. For these, abnormal respiratory patterns are used to “reset” the system instead of the classic DTR, as well as other brain nuclei such as the basal ganglia to regulate motor system responses.
Specific diagnostic, stimulation, and treatment tools have been developed for the 12 pairs of cranial nerves (involved in sensory, motor, and visceromotor functions), enabling treatment of many neurological dysfunctions and symptoms. Manual Muscle Testing and specific stimuli applied to a particular nucleus serve to assess the CNS’s normal or abnormal response in order to trace the primary dysfunction and the brain’s compensatory strategies for each cranial nerve dysfunction.
Once the evaluation is complete, the P-DTR protocol is used to confirm the dynamic context. When primary and secondary dysfunctions are clearly identified, both dysfunctions are simultaneously stimulated together with the appropriate abnormal respiratory pattern, thus enabling effective CNS resetting.
Currently, the P-DTR method is the subject of extensive research and study. Preliminary electroneuromyographic investigations conducted by the Department of Neuroscience, Physiotherapy, and Reflex Therapy at the Smolensk State Medical University have clearly demonstrated the interrelation between primary dysfunctional and compensatory receptor fields, confirming the hypothesis of paired signals.
To analyze the state of central nociceptive and antinociceptive mechanisms, the exteroceptive suppression method was employed, revealing a reduction in inhibitory interneuron activity at the brainstem level, which mediates nociceptive responses. This suggests that P-DTR treatment affects not only the peripheral component of pain but also the central antinociceptive structures that help reduce the pain syndrome.
To assess the state of autonomic skin responses in patients before and after P-DTR treatment, the sympathetic skin potential was measured pre- and post-treatment. In most cases, the patient’s sympathetic skin response significantly decreased.
After observing a large number of patients treated with the method, it was concluded that in some cases, P-DTR can be used as a standalone treatment, enabling patients to restore correct biomechanics and resolve many problems without medication. In other cases, P-DTR can serve as a complementary treatment alongside medications, therapeutic, or surgical procedures. It is evident that P-DTR treatment helps restore proper proprioception, achieve normal tonicity in certain muscle groups, improve posture, eliminate antalgic postures, align gait, and enhance the effectiveness of therapeutic treatments such as physiotherapy and others.